 Cryoablation · NYC
Cryoablation · NYC
Cryoablation for Prostate Cancer
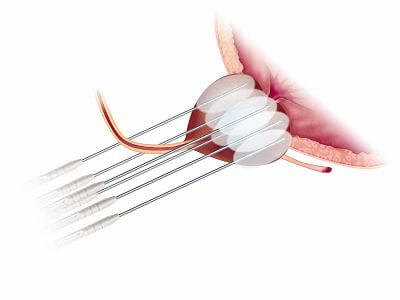
Prostate cryoablation can be performed as a focal or partial-gland treatment, using thin cryoprobes placed through the perineum to freeze the targeted cancer-bearing region of the prostate. Treatment temperatures are commonly targeted around −40°C in the cancer-bearing region, with thin probes placed under ultrasound guidance and MRI/ultrasound fusion planning used to target the MRI-visible lesion. A urethral warming catheter protects urinary structures throughout the procedure.
Dr. Tan tailors the ablation pattern to the tumor location, with the goal of treating the cancer-bearing region while preserving uninvolved prostate tissue, neurovascular structures, and urinary function whenever oncologically appropriate. He also performs salvage cryoablation for men with biopsy-proven recurrence after radiation therapy, one of the situations where cryoablation is often considered as a less invasive alternative to salvage prostatectomy.
“For the right patient, partial-gland cryoablation can provide durable intermediate-term cancer control while preserving urinary and sexual function.”- Dr. Wei Phin Tan, MD, MHS, FACS
Dr. Tan's Cryoablation Protocol
- Selected intermediate-risk prostate cancer with an MRI-visible dominant lesion or region of disease confirmed by biopsy mapping
- Several representative ablation patterns: quadrant, hemiablation, anterior, hockey-stick, and subtotal, rotated or modified to match the patient's MRI and biopsy map
- Two-cycle rapid freeze with treatment temperatures commonly targeted around −40°C in the cancer-bearing region, with thermocouple monitoring
- Urethral warming catheter to protect urinary function
- Follow-up: PSA every 6 months; MRI at 6–12 months, 2 years, 3.5 years, and 5 years
Representative Ablation Patterns
Dr. Tan uses several representative ablation patterns, including quadrant, hemiablation, anterior, hockey-stick, and subtotal approaches, which can be rotated or modified to match the patient's MRI and biopsy map. The illustrations below show example geometries; in practice each pattern is adapted to the individual tumor.
How to read these diagrams: each image is an axial (cross-sectional) view of the prostate. Top = anterior (pubic bone side). Bottom = posterior (rectum side). The gray extensions on either side are the neurovascular bundles. The central white oval is the urethra. The dark red shape is the tumor. The dashed line marks the planned ablation boundary.
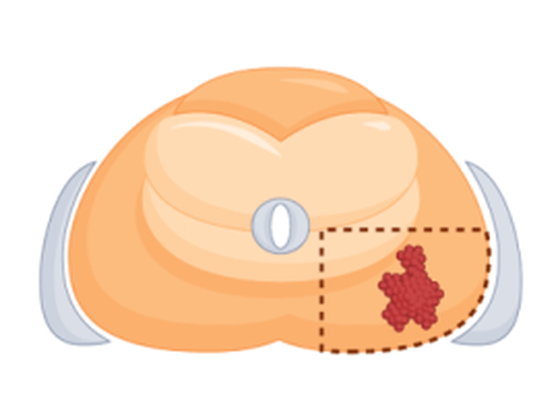
Quadrant Ablation
Example: posterolateral quadrant. Treats one of the four quadrants when cancer is confined to a single corner of the gland.
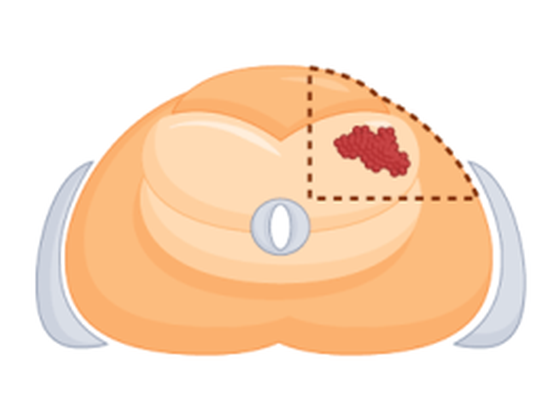
Quadrant Ablation
Example: anterolateral quadrant. Same pattern applied to the anterior zone, a region often missed by transrectal biopsy but reliably mapped on MRI.
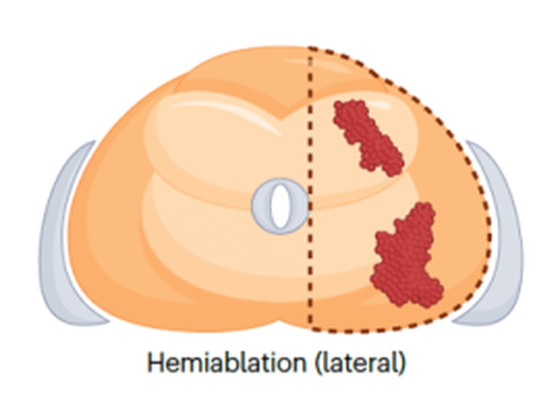
Hemiablation, Lateral
Ablates an entire left or right half of the prostate when cancer is lateralized to one side.
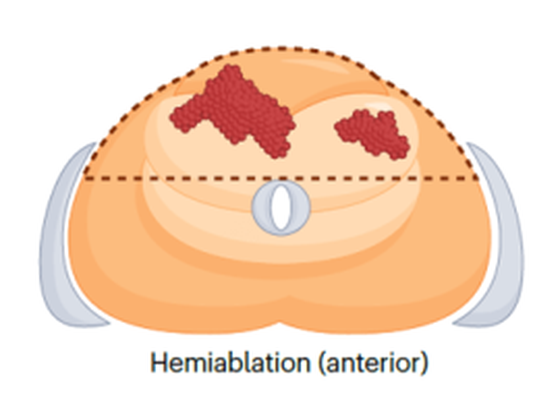
Hemiablation, Anterior
Covers the full anterior half of the gland when disease spans the front but spares the posterior zone and rectum.
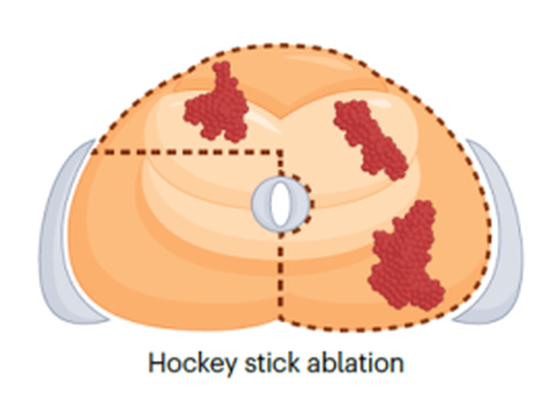
Hockey-Stick
An L-shaped freeze zone that combines the anterior band with one lateral side, used when the tumor wraps across two zones.
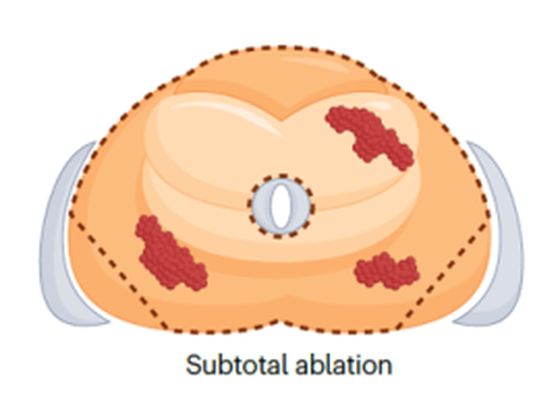
Subtotal Ablation
Treats most of the gland while deliberately sparing a margin near one neurovascular bundle, used for larger, multifocal disease.
Note: these images are illustrative. Dr. Tan's planning software mirrors or rotates each pattern to match your own MRI and biopsy map, so the actual ablation conforms to your tumor, not the other way around.
Key Advantages
- Real-time ice ball monitoring, visualize the ablation as it happens
- Urethral warming catheter protects urinary structures
- Established platforms with decades of urologic data
- Future options remain open, repeat focal therapy, radiation, or surgery may still be possible if cancer recurs, depending on the recurrence pattern and prior treatments
Cryoablation vs HIFU: How Dr. Tan Chooses
Cryoablation and HIFU are both focal therapies for localized prostate cancer, but they treat the prostate in opposite ways. Cryoablation uses extreme cold to freeze and destroy the cancer-bearing region; HIFU uses focused ultrasound heat. Because Dr. Tan performs both, the choice is driven by tumor location, prostate anatomy, and prior treatment, not by which device is available.
- Anterior tumors: cryoablation is generally preferred because the ice ball can reliably reach the front of the prostate, while HIFU has limited acoustic penetration to the anterior gland
- Larger prostates: cryoablation can ablate a larger volume in a single session, whereas HIFU treatment time scales with prostate size
- Posterior, mid-gland, or smaller prostates: HIFU is often preferred when the tumor sits within the optimal acoustic window of the rectal probe
- Calcifications: dense prostate calcifications can block HIFU energy; cryoablation is unaffected
- Salvage after radiation: cryoablation has the longest track record and is the more common option, although HIFU can also be considered in selected cases
- Side-effect profile: both treatments may affect urinary and erectile function. The risk profile depends on tumor location relative to the urethra, neurovascular bundles, and rectum
For most patients, the better question is not "cryo or HIFU?" but "what does the MRI show, where is the tumor, and which approach gives the best chance of cancer control while preserving function?" Dr. Tan reviews each case individually and discusses both options when both are reasonable.
Salvage Cryoablation After Radiation for Prostate Cancer in NYC
Salvage cryoablation after radiation for prostate cancer in NYC is offered by Dr. Tan for men with biopsy-proven local recurrence after prior radiation therapy. When prostate cancer comes back after radiation, the first step is to prove that the recurrence is truly local. A rising PSA alone is not enough. Dr. Tan confirms recurrence with modern imaging, usually PSMA PET and prostate MRI, followed by targeted biopsy when appropriate. The goal is to distinguish cancer that is still confined to the prostate from cancer that has already spread elsewhere.
For carefully selected men with biopsy-proven local recurrence after radiation, salvage cryoablation can offer a second chance at local control without removing the prostate. Thin cryoprobes are placed through the perineum and used to freeze the recurrent tumor, while a warming catheter protects the urethra. Depending on the location and extent of recurrence, treatment may be focal, hemi-gland, subtotal, or whole-gland.
Salvage cryoablation is often preferred over salvage prostatectomy because surgery in a previously radiated field is technically difficult and associated with higher risks of urinary leakage, bladder neck scarring, rectal injury, and erectile dysfunction. Cryoablation is still a real treatment with real risks, but it is less invasive and can be tailored to the area of recurrence.
Who may be a candidate?
Salvage cryoablation may be considered when:
- PSA is rising after prior radiation therapy
- PSMA PET and MRI suggest recurrence is confined to the prostate
- Biopsy confirms local recurrent prostate cancer
- There is no evidence of metastatic disease
- The recurrent tumor can be safely targeted
- The patient wants local treatment but wants to avoid the morbidity of salvage prostatectomy
Why cryoablation after radiation?
Radiation changes the prostate and surrounding tissues. Planes are scarred, healing is less predictable, and surgery becomes more difficult. Cryoablation avoids dissecting around the prostate and instead treats the recurrence from within the gland. This makes it an important option for men with localized radiorecurrent prostate cancer.
Important Counseling Point
Salvage cryoablation is not the same as primary cryoablation. Because the prostate has already been radiated, the risk of urinary symptoms, erectile dysfunction, urethral scarring, urinary retention, and rare rectal complications is higher than in men having focal cryoablation as their first treatment. Careful patient selection and precise treatment planning are essential.
Dr. Tan's Approach
Dr. Tan evaluates each patient with PSA history, prior radiation records, MRI, PSMA PET, and biopsy mapping. The ablation plan is then customized to the recurrence pattern, whether that means focal treatment, hemiablation, subtotal ablation, or whole-gland salvage cryoablation. The goal is to treat the recurrent cancer while minimizing additional injury to urinary, sexual, and rectal structures.
Selected Evidence (Dr. Tan's Published Work)
Dr. Tan has published extensively on prostate cryoablation, including primary partial-gland and salvage outcomes. Selected first-author and senior-author papers:
- Tan WP, Wysock JS, Lepor H. Partial gland cryoablation for prostate cancer, where are we? Nature Reviews Urology. 2023. PMID 36434111
- Tan WP, Kotamarti S, Chen E, et al. Oncological and functional outcomes of primary whole-gland cryoablation, 20-year experience. Cancer. 2022. PMID 36107496
- Tan WP, Kotamarti S, Ayala A, et al. Oncological and functional outcomes for salvage whole-gland cryoablation. European Urology Oncology. 2023. PMID 36890104
- Tan WP, Chang A, Sze C, et al. Individualized partial gland cryoablation outcomes. Journal of Endourology. 2021. PMID 33559527
- Tan WP, ElShafei A, Aminsharifi A, et al. Salvage focal versus whole-gland cryotherapy comparison. Clinical Genitourinary Cancer. 2020. PMID 31892490
- Lee H, Thakker S, Pineault K, et al. Salvage cryoablation for recurrent prostate cancer following radiation. Cancers. 2024. PMID 39123445
- Ghoreifi A, Hussain J, Tan WP, et al. Comparative effectiveness of partial gland cryoablation vs robotic radical prostatectomy. European Urology Focus. 2025. PMID 39893046
Full publication list pulled live from PubMed on the Publications page.